Instructions: Select NCCN Risk Group to view the corresponding report.
Very Low/Low
Favorable Intermediate
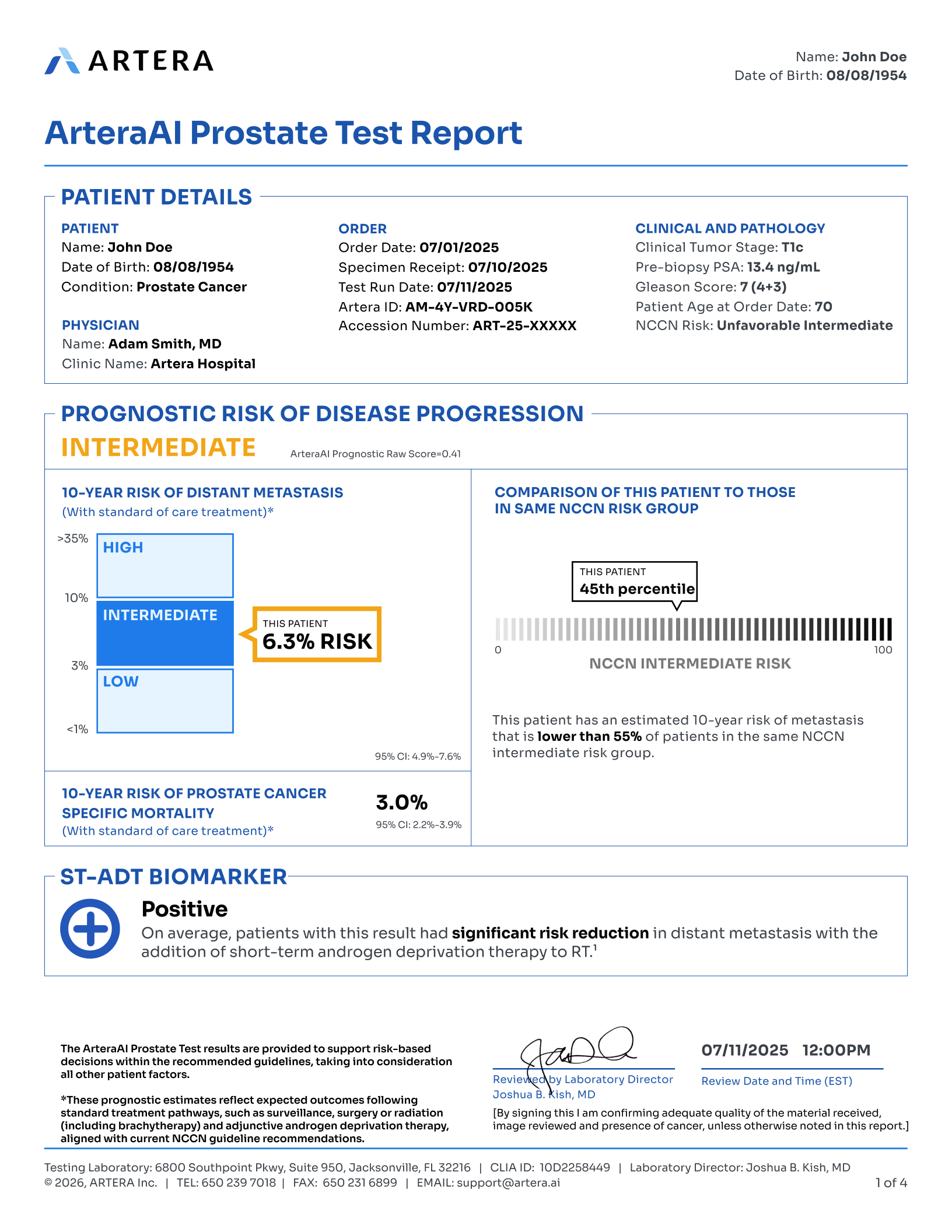
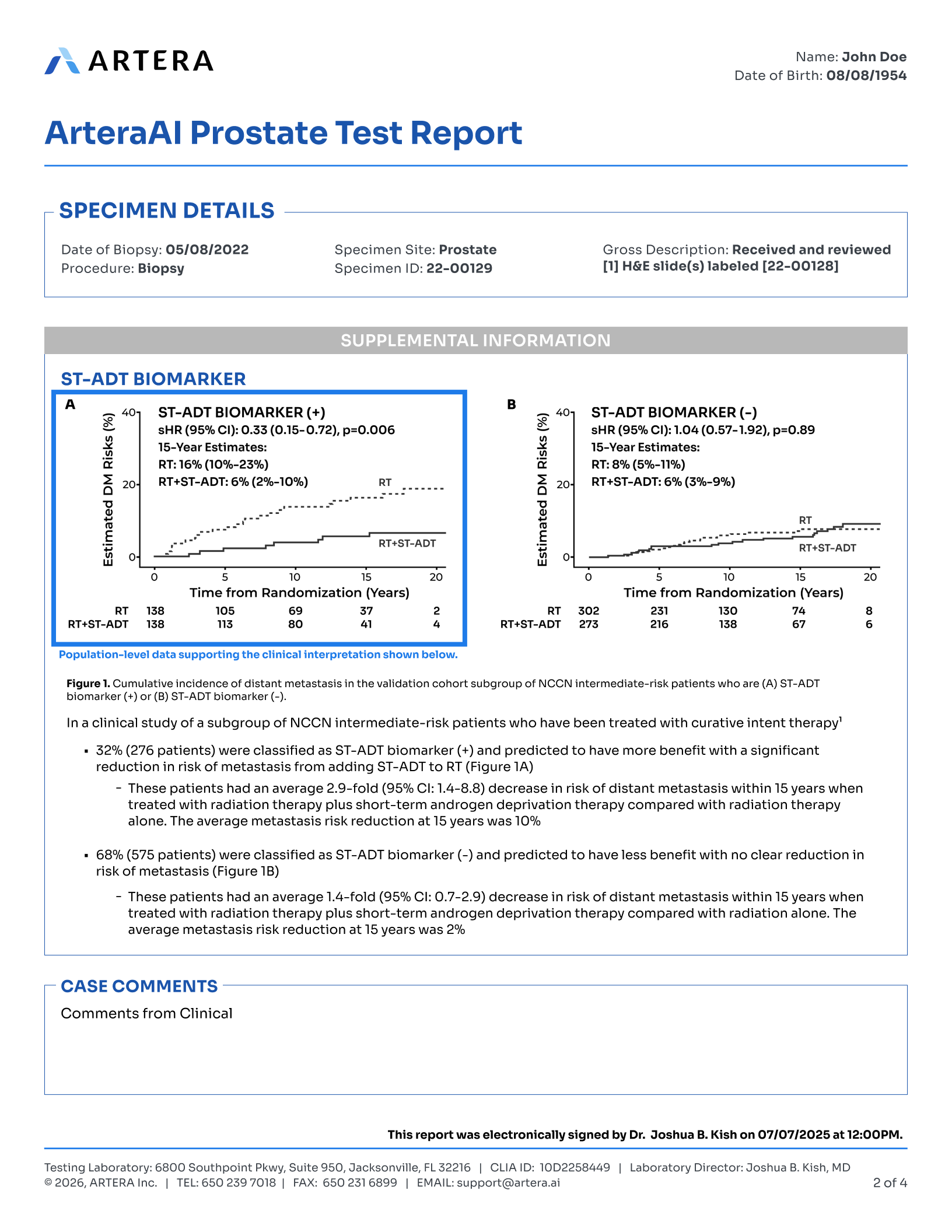
Unfavorable Intermediate
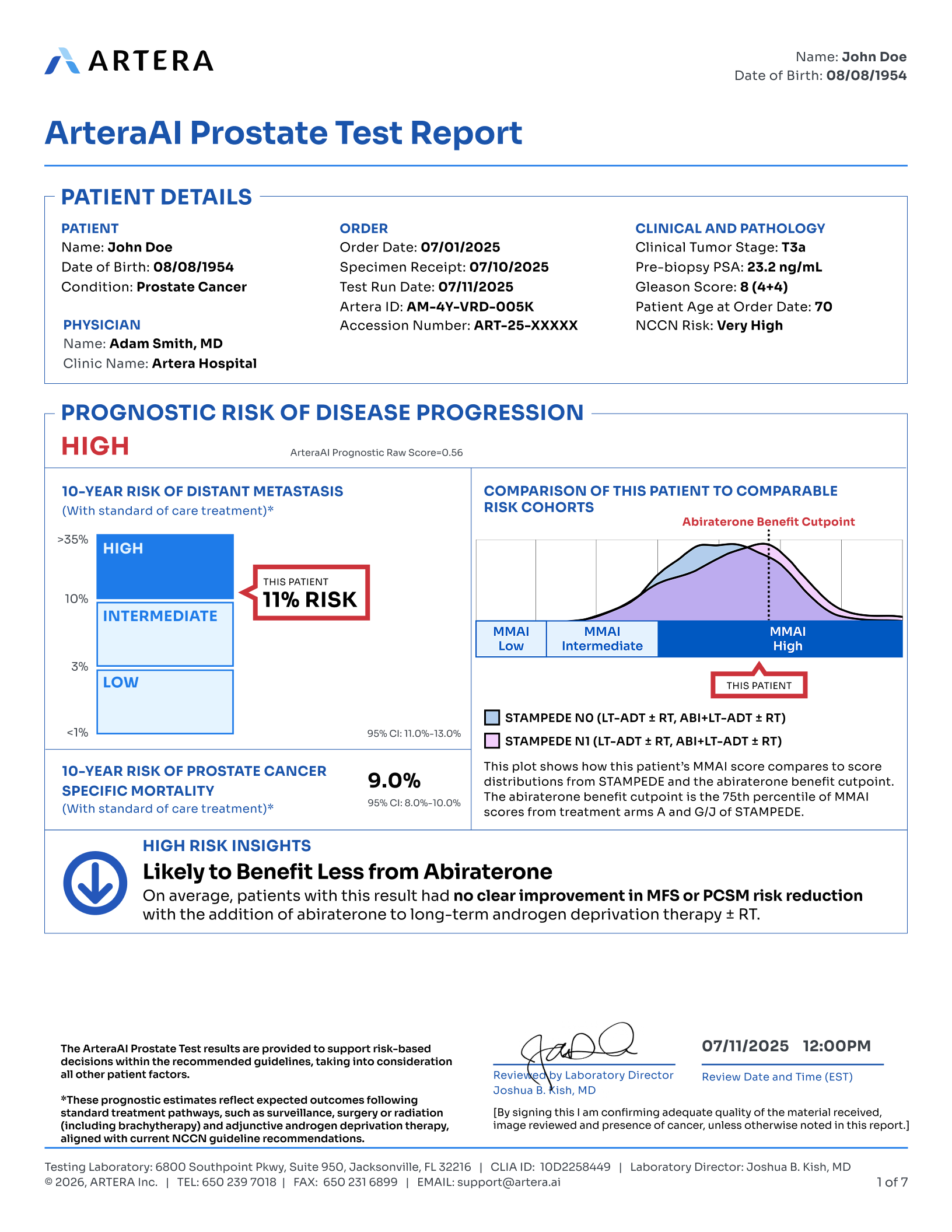
High/Very High
Instructions: Select NCCN Risk Group to view the corresponding report.